
With bracketless fixed orthodontics, no one will notice your braces.
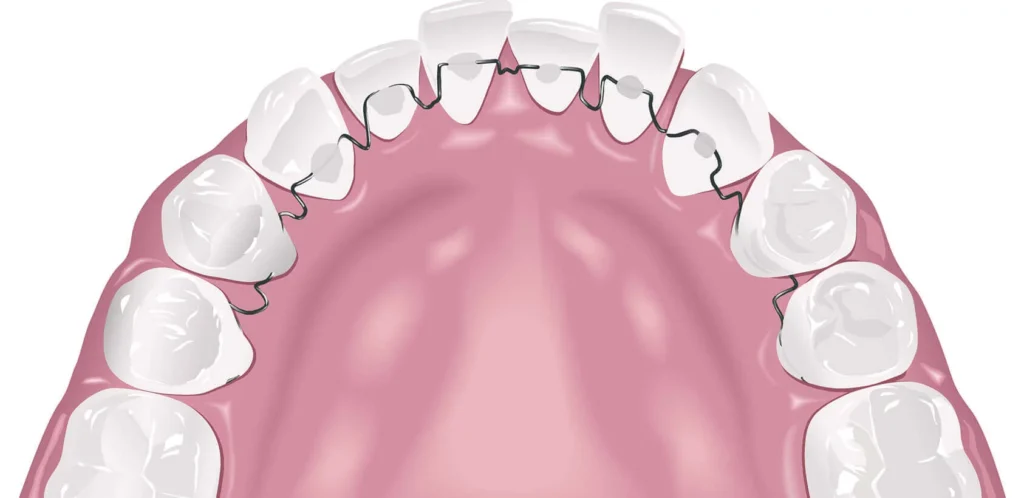
Bracketless fixed orthodontics is a branch of orthodontics that involves placing braces (brackets and wires) on the inner surface of the teeth, the side facing the tongue, instead of on the outer (vestibular) surface as with traditional braces. The appliance is virtually invisible.

Naturally invisible
Bracketless fixed orthodontics is truly invisible when you smile and speak, unlike common clear aligners. This is a major benefit of the treatment.

No speech problems
Fixed orthodontic appliances with lingual brackets can cause speech and pronunciation issues. With this therapy, this doesn’t happen.

No pain or discomfort
This treatment, which can be used to correct any type of malocclusion, is virtually painless, both during application and afterward.
No more placing, metal or ceramic braces on your teeth.
What is bracketless fixed orthodontics?
Bracketless fixed orthodontics is the most innovative orthodontic treatment available. Compared to traditional bracket-based systems, nothing changes in terms of diagnosis, treatment planning, results, or treatment duration. What is truly innovative is the type of appliance used. It is the most requested orthodontic treatment among patients who care about aesthetics and comfort, as the appliance is not only invisible but also extremely thin.




The invisibility of bracketless fixed orthodontics available at Studio Dentistico Cozzolino is due to its position: the orthodontic wires are bonded to the non-visible inner surface of the teeth. This system works without brackets, the classic metal or ceramic buttons used in traditional orthodontic treatments. This helps patients avoid the embarrassment and anxiety often associated with wearing visible orthodontic appliances.
The bonding procedure for bracketless devices follows standard protocols, is not painful, and does not weaken or damage the teeth or gums. There is no pain when the wires and bonding material are removed, and the procedure is carried out with full respect for dental and periodontal health.
The invisible appliance used in bracketless fixed orthodontics goes beyond clear aligners and allows the appliance to remain completely hidden from the view of others. It is perfect for those who need an unchanged smile, perfect pronunciation, and a harmonious appearance with teeth free from brackets of any kind. Virtually imperceptible, since it is positioned behind the teeth, the invisible appliance allows the correct shape and alignment of the upper and lower arches to be restored without affecting aesthetics.

Orthodontist Dr. Anna Mariniello specializes in Orthodontics and Gnathology and is an expert in bracketless fixed orthodontics. She is the co-author, together with Dr. Fabio Cozzolino, of the The Atlas of Bracketless Fixed Lingual Orthodontics
Difference from other orthodontic treatments
When people talk about invisible treatments, they refer to those positioned on the non-visible surfaces of the teeth, and lingual brackets also fall into this category. However, because of their complex shape, they are more noticeable to the tongue: in addition to causing irritation, they may affect speech. These discomforts are absent in bracketless treatments, where speech alterations are rare and usually limited to the first few hours after starting treatment.
To achieve perfection, which is often the goal of patients seeking the best aesthetic result, it may be necessary to modify the shape and color of certain teeth. This can be achieved through a multidisciplinary approach involving composite restorations or dental veneers.
Therefore, bracketless fixed orthodontics therapy is invisible and the most comfortable solution available: it works without brackets and therefore without protrusions that could irritate the tongue or affect speech. With this technique, all types of malocclusions can be corrected with treatment times and results similar to those achieved with bracket-based therapies.
Dental aligners, also called trays, should be considered more aesthetic than traditional brackets, but not truly invisible treatments. Aligners are especially noticeable at the beginning of treatment when the teeth are severely misaligned. They create a plastic-film effect on the teeth, and in most cases fixed composite buttons (attachments) are required, without which certain tooth movements would not be possible. Their visibility decreases when the teeth become more aligned and in the absence of attachments.


Preliminary phase of bracketless fixed orthodontics
The pre-treatment study consists of diagnosing the malocclusion and choosing the therapeutic strategy, also based on the patient’s needs. It takes into account important radiographic and clinical parameters. The main radiographs examined are the panoramic X-ray of the dental arches and the lateral cephalometric X-ray of the skull. These examinations provide information about the position, number, anatomy, and health condition of the teeth, their position within the bones, and the relationship between the skeletal bases.
The clinical analysis concerns both the condition of the dentoalveolar arches, the periodontal examination, and the possible presence of cavities. The clinical evaluation also includes the study of facial aesthetics, with particular attention to the position of the teeth in relation to the lips and the center of the face.
How bracketless fixed orthodontics treatment is performed
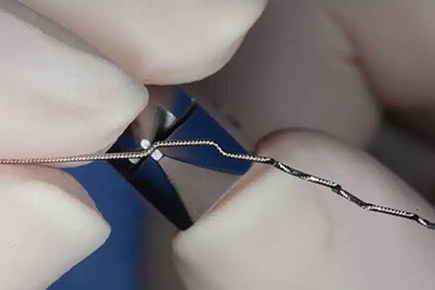
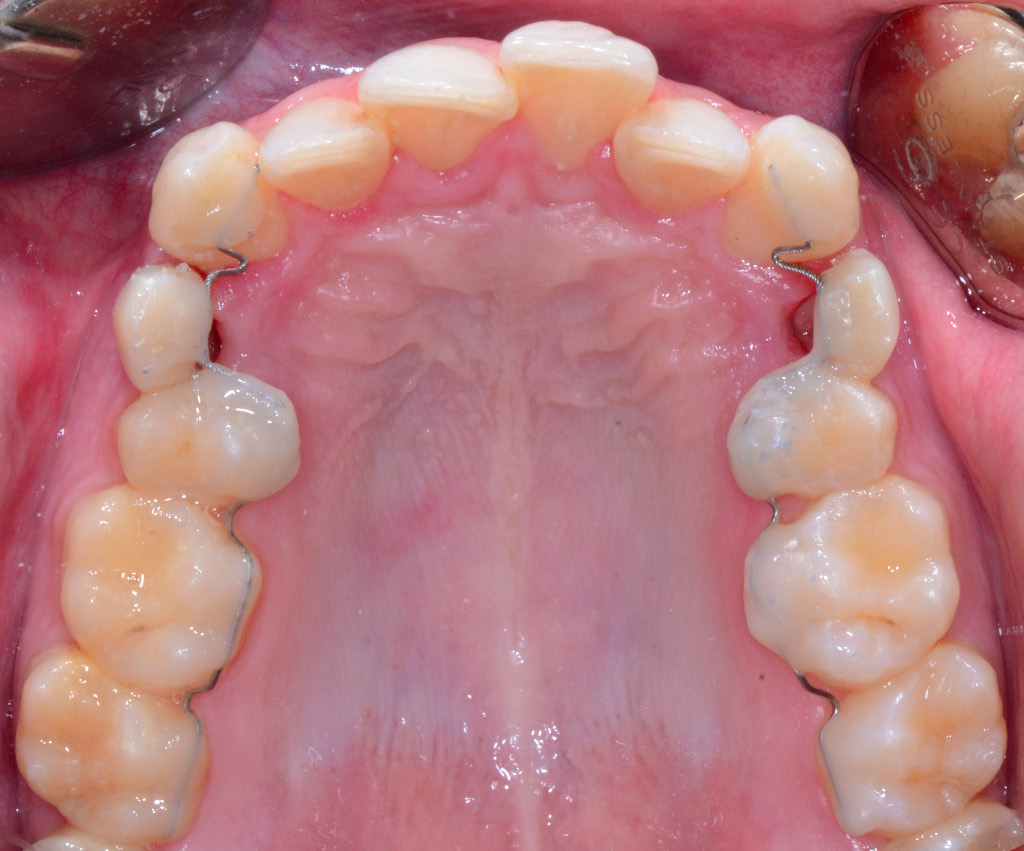
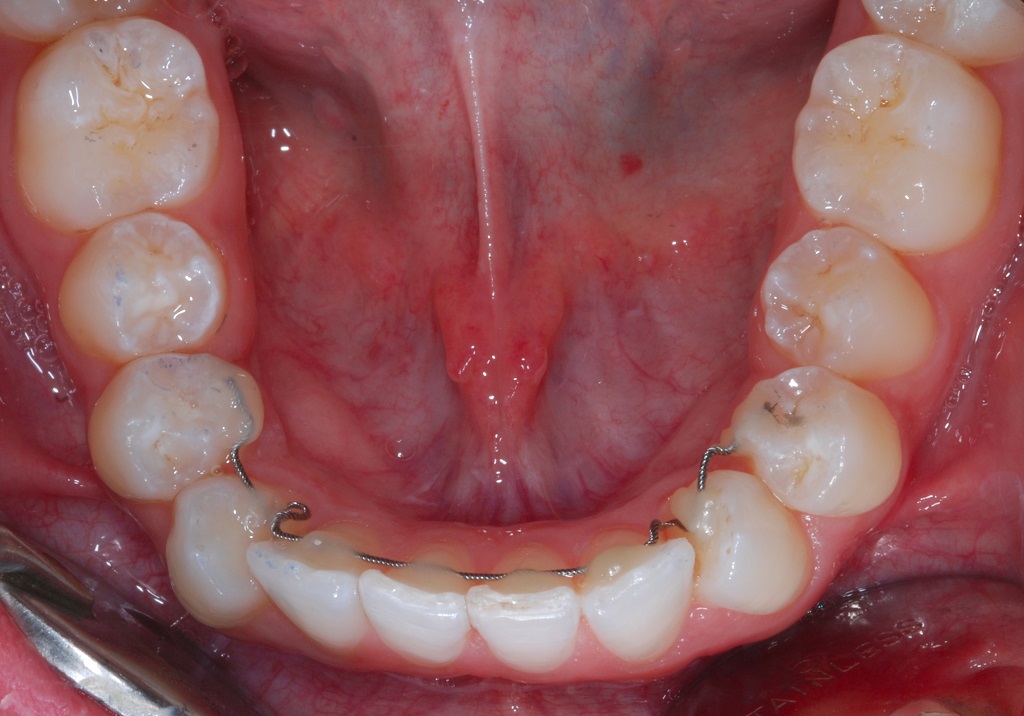
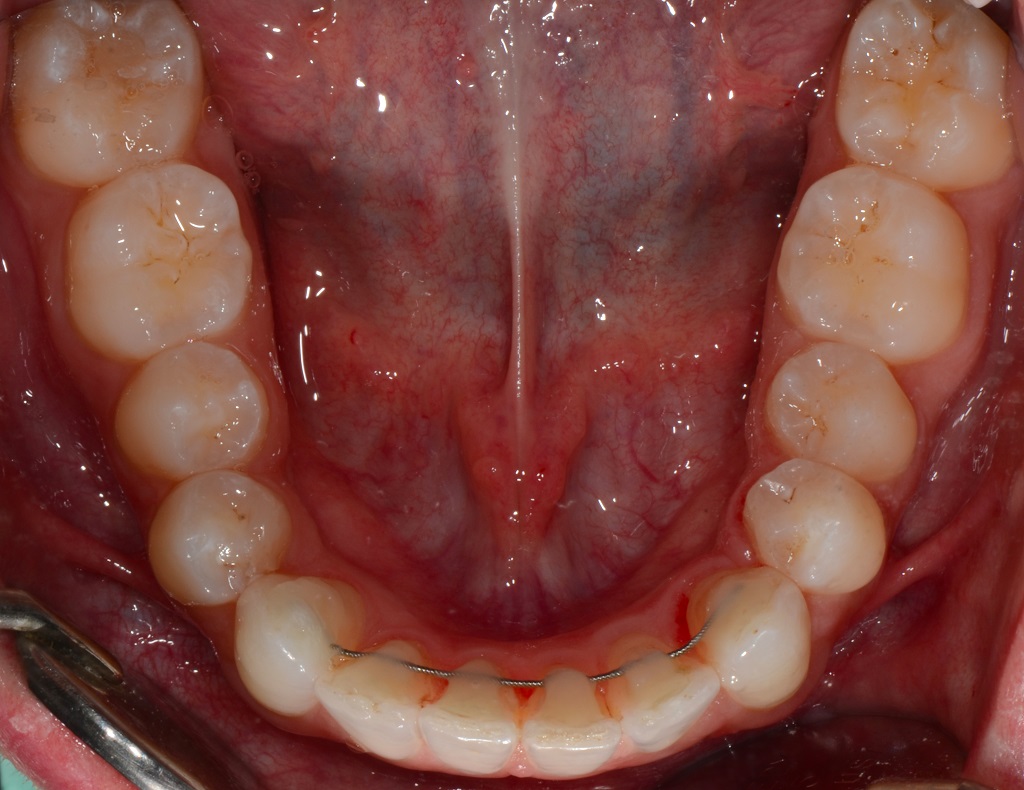
The treatment known as invisible lingual orthodontics uses very thin wires, approximately 1 mm thick, to place the invisible orthodontic appliance. The most commonly used are Nickel-Titanium (Ni-Ti) arches and braided steel wires, the classic splinting wires used to stabilize teeth with fixed retainers at the end of traditional orthodontic treatments with brackets (passive retainers).
The braided steel wires are meticulously shaped according to the anatomy of the teeth and the movements that need to be achieved. So, how is a bracketless treatment performed? It is a procedure that is:
- Customized
- Precise
These wires for the invisible appliance must be shaped to achieve the desired tooth movement and obtain perfect dental alignment. The shaping process is extremely precise and individualized, allowing both perfect adaptation of the wire to the tooth anatomy and the achievement of the desired movement.
It is also essential for obtaining correct alignment. The dentist providing the invisible appliance uses Ni-Ti arches, and during bonding, the activations are achieved through the meticulous adaptation between the wires and the teeth. Therefore, in bracketless fixed orthodontics, the wires are not pre-shaped but modified during the bonding phase on the teeth, taking into account both tooth anatomy and the required movements.
How is the metal orthodontic wire positioned? The surfaces involved in bonding are first treated with a gel that is suctioned away after a few seconds and then rinsed thoroughly with water. This is followed by the application of an adhesive layer, which is polymerized — fixed using a curing light — after which the wires are bonded using a fluid composite material that hardens and adheres firmly to the teeth thanks to the action of the light.
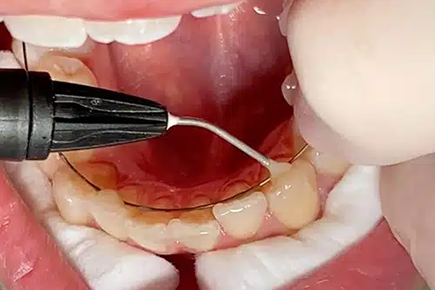



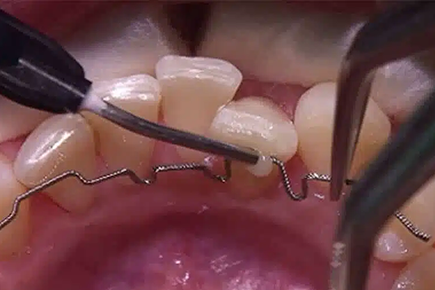


The adaptation of the wires to the teeth is so precise and anatomical that it almost seems as if they slide within grooves carved into the teeth, although this is obviously not the case, since they are, as already explained, simply placed against the teeth and covered with a thin layer of composite material. In these images, you can see the sequence of photographs illustrating how bracketless fixed orthodontic appliances are applied, including all the steps involved in the procedure.
Our knowledge is collected in the Atlas
In the field of contemporary orthodontics, bracketless fixed orthodontics represents one of the most significant evolutions of recent years. Dr. Anna Mariniello and Dr. Fabio Cozzolino were the ones who systematized this technique and introduced it to the scientific community through the Atlas of Bracketless Fixed Lingual Orthodontics, published by Quintessenza Edizioni.
With this volume, Dr Mariniello and Dr Cozzolino provided the dental community with a comprehensive scientific reference on a technique that, although originally developed as a solution for relapse problems, has established itself as an independent therapeutic approach capable of treating a wide range of malocclusions in a completely invisible and highly comfortable way.
More information about the Atlas of Bracketless Fixed Lingual Orthodontics
What happens after the appliance is applied
After a few days, patients report that they no longer feel the appliance and that they adapted to it very quickly. Only in very few cases, usually involving severe malocclusions, does the patient continue to notice its presence, even though it remains comfortable. During follow-up appointments, reactivation of the device may be necessary by detaching it from some teeth in order to reactivate it (a painless and safe procedure for the patient), or the wire may need to be completely replaced, just as in traditional orthodontic treatments with brackets.
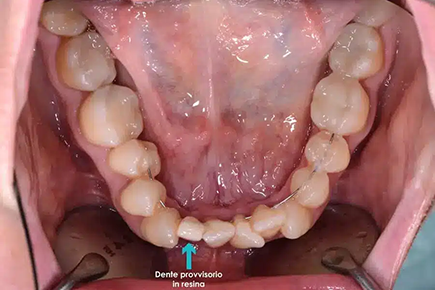
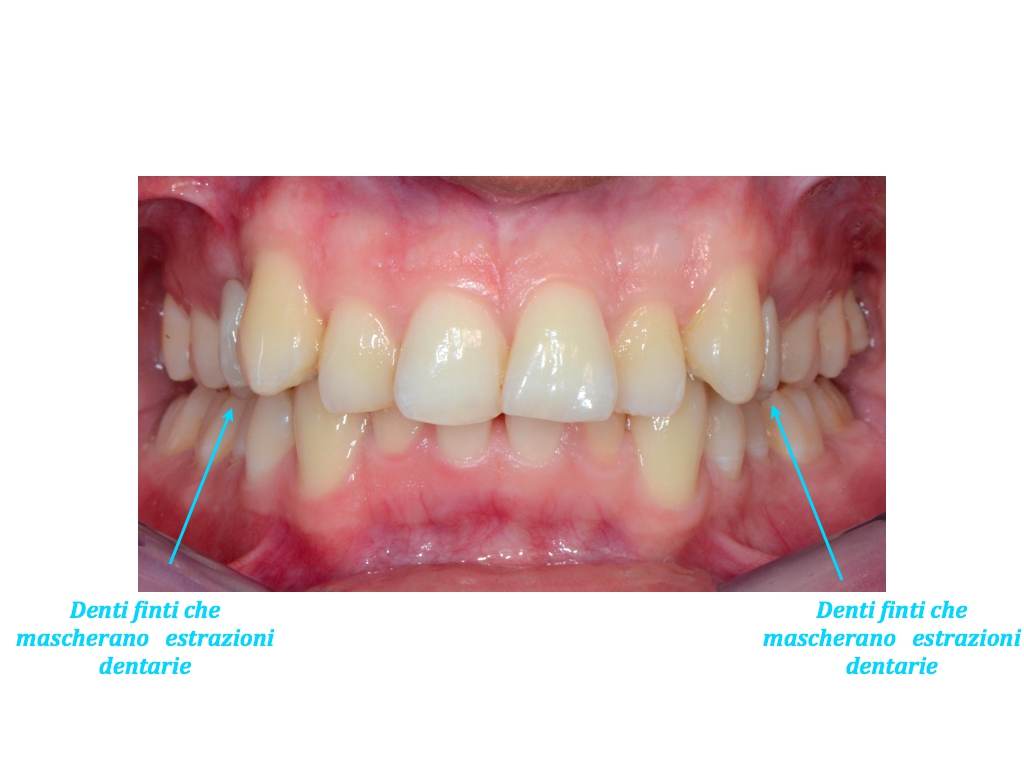
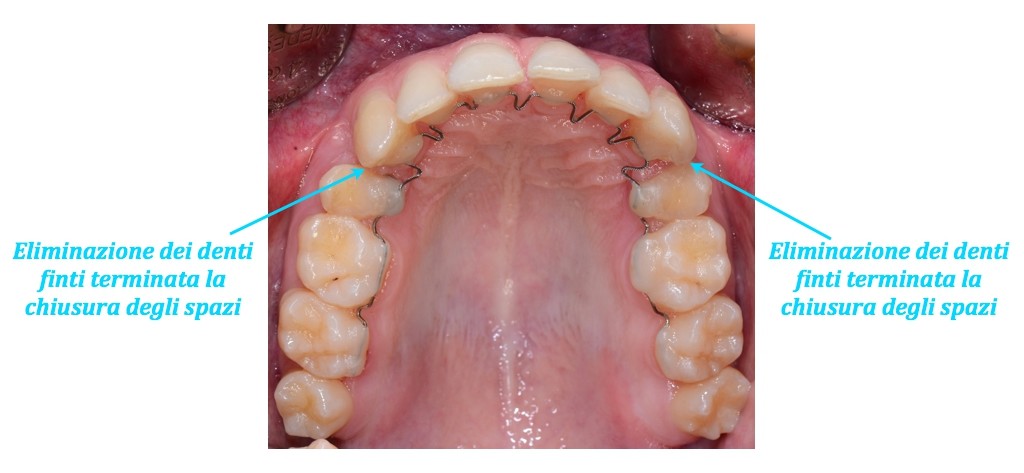
Some malocclusions require the extraction of one or more teeth in order to be corrected. For this reason as well, invisible lingual bracketless fixed orthodontics should be supported by a multidisciplinary approach. At Studio Dentistico Cozzolino, extractions are often performed by Dr Fabio Cozzolino, who perfected the Extraction Without Forceps (EWF) technique for all teeth, including the atraumatic extraction of wisdom teeth. In cases of orthodontic extractions, it is possible to conceal the absence of the extracted teeth using resin replacement teeth attached to the orthodontic wires. These teeth closely match the shape and color of the extracted teeth, making their absence virtually imperceptible. This applies to all types of extractions, for example first premolars or baby canines (when extracted to allow the permanent tooth to erupt).
Oral hygiene and diet with the invisible appliance
During any fixed orthodontic treatment, it is essential for the patient to maintain meticulous oral hygiene at home and to be careful with their diet. The appliance itself does not cause cavities; however, it makes the removal of plaque and food debris more difficult. In addition to brushing the teeth after every meal (a recommendation that is always valid even without an appliance), it is necessary to use additional tools such as a water flosser (a jet of water that helps remove food debris and plaque even from undercuts and interdental spaces), dental floss, superfloss (a dental floss with a rigid end to facilitate insertion followed by a spongy section), interdental brushes, and similar aids.
The professional will recommend the most effective tools for each individual case to ensure proper cleaning. Regarding diet during lingual orthodontic treatment, it is necessary to avoid particularly hard foods such as rustic bread, nougat, hard wheat biscuits, as well as sticky chewing gum and candies, both to prevent detachment of the appliance and for hygiene reasons.
Reasons to choose invisible orthodontics
Among the advantages of bracketless fixed orthodontics are complete invisibility on both the upper and lower arches, no discomfort, and no speech alterations caused by a foreign body. Unlike lingual brackets, which also allow invisible treatment, tongue discomfort and speech alterations with bracketless fixed orthodontics are rare events and, in any case, limited to the first few hours after the appliance is applied.
The appliance is thinner and has no protrusions that could injure the tongue. This treatment is invisible and extremely comfortable, allowing the correction of all types of malocclusions (Angle Class I, II, and III, open bite, deep bite, scissor bite, gummy smile, etc.).
Opinions on invisible orthodontics
- Completely invisible appliance.
- No pain during or after the procedure.
- No speech problems.
- Treatment suitable for every type of malocclusion.
- Comfortable and convenient over time.
Opinions on traditional orthodontics
- Visible appliance on the teeth.
- Presence of speech alterations.
- Bulky during chewing.
- More difficult oral hygiene.
- Uncomfortable in daily life.
The advantage of bracketless fixed lingual invisible orthodontics also lies in the high level of comfort for the tongue and oral tissues. Since it is free of brackets, it is very thin and therefore suitable for all patients who need a treatment that is not only invisible but also barely noticeable, almost as if they were not wearing an appliance at all. There are no speech alterations, and tongue or mucosal discomforts are rare and quickly resolved.
Difference between invisible orthodontics and clear aligners
When people talk about invisible orthodontics, they often refer to clear aligners, commonly called alignment trays. Aligners are less visible than traditional metal or ceramic vestibular brackets and create the optical effect of a transparent film visible on the teeth. Numerous studies on clear aligners are available in scientific literature.

While aligners are removable, meaning they can be taken out but must be worn 22 hours a day to remain effective, bracketless lingual orthodontics is an invisible technique that uses a fixed appliance. Removable aligners are generally more suitable for mild dental misalignments, whereas a fixed appliance is essential in cases of more severe malocclusions or significant misalignments. The advantage of wearing an invisible fixed appliance without brackets is not only aesthetic: it also greatly reduces the anxiety associated with difficulties in eating or speaking, as well as the embarrassment of appearing in public with a visible orthodontic appliance.
Removable appliances such as clear aligners may not be able to correct malocclusions with the same precision as a fixed appliance, and this can increase the risk of post-treatment relapse. In practice, the teeth may become misaligned again, returning to their original crooked position. After an accurate diagnosis, the orthodontist who uses invisible appliances will be able to recommend the most suitable treatment and determine whether the malocclusion requires a fixed appliance or can also be corrected with removable appliances such as aligners.
Bibliographic references on the use of clear aligners.
Djeu G, Shelton C, Maganzini A. (Outcome assessment of Invisalign and traditional orthodontic treatment compared with the American Board of Orthodontics objective grading system) showed that invisible aligners “did not treat malocclusions as well as braces”. Uribe F, Cutrera A, Nanda R (A segmented appliance for space closure followed by Invisalign and fixed appliances.) assert that the aligners are deficient in their “ability to correct large anteroposterior discrepancies and occlusal contacts”.
Giancotti A, Greco M, Mampieri G (Extraction treatment using Invisalign Technique) say that with the invisible aligners “the space closure achieved with crown tipping and without correct root inclination making a further fixed appliance phase necessary”. According to Uribe F, Cutrera A, e Nanda R, this fixed appliance phase may also be necessary due to the limitations of transparent aligners “in achieving rotational and vertical movements”.
Studies carried out by Kuncio D, Maganzini A, Shelton C, and Freeman K (Invisalign and traditional orthodontic treatment postretention outcomes compared using the American Board of Orthodontics objective grading system.) demonstrate, in their group of patients, that those treated with the aligners “relapsed more than those treated with conventional fixed appliances”.
Studies by Nedwed V and Miethke RR show that patients accept more easily be treated with masks that with lingual brackets because they consider the therapy less annoying.
Clinical cases dedicated to bracketless lingual orthodontics
Some clinical cases of dental malocclusions treated at Cozzolino Dental Office by Dr. Anna Mariniello using the technique of bracketless fixed orthodontics.
A female adult patient wanted to solve the lack of contact and protrusion of her teeth.
A conventional visible appliance with brackets would have caused a considerable embarrassment, while the application of a lingual device with brackets, even though not visibile, made her anxious because of the risk of fastidious irritations of the tongue as well as phonetic alterations. Therefore, the therapy was realized using lingual bracketless orthodontics, nowadays the most thin appliance available.






The therapy was performed using invisible lingual bracketless orthodontics, with the application of intermaxillary rubbers, that the patient puts on by himself.
The hooks for the rubbers, attached on the external surfaces of the teeth in order to make their application easier for the patient, in visible areas were realized with ceramic material, so that they were completely camouflaged.












To correct the malocclusion, it was necessary to extract superior premolars. The therapy was done by means of invisibile lingual bracketless orthodontics and the dental extractions were not evident thanks to the presence of fake resin teeth attached to the lingual appliance. These teeth were worn till they were completely removed when the space created by the extractions was filled up by the remaining aligned teeth.





An adult patient presented with a milky canine in the maxillary arch, while the permanent tooth was included in the bone. The therapy was done in a completely invisibile way through the use of lingual bracketless orthodontics. The extraction of the milky canine and the positioning of the hook on the included tooth were performed under local anesthesia, in a completely painless way for the patient.
The space obtained from the extraction of the milky canine was masked with a fake resin canine, kept in place till the permanent tooth was correctly placed in the arch.









A 28-year old female patient presented with maxillary crowded teeth, the right canine in ectopic position and the mandibular midline moved on the right side.
The patient requested for a comfortable and invisible therapy, without phonetic alterations and problems to the gums. Therefore, the malocclusion was treated with lingual bracketless orthodontics.
After the application of the retainers, the patient was monitored every 3-4 weeks.
Dental alignment was obtained after about 10 months, with complete satisfaction of the patient. Then, the active retainers were substituted with passive ones.






The dental alignment and the resolution of the cross bite of the left lateral incisor were made with lingual bracketless orthodontics at both arches.





No more braces that ruin your smile
Questions and answers about bracketless fixed orthodontics
Yes, but only to reposition natural teeth, since implants cannot change their position because of osseointegration.
The bonding procedure follows traditional protocols and, in addition to not being harmful, it is not painful either. Everything is carried out with full respect for the health of the teeth and gums. As with all fixed appliances, patients are advised to avoid hard foods.
So it is clear that orthodontic therapies play a fundamental role not only for esthetics or periodontal health, but also for the general health of our organism as well as for a complete psychophysical wellness.
No. At the end of treatment, the adhesives used to bond the appliance are selectively removed using special burs that do not damage the tooth surface and cause no pain. In some cases, after alignment, certain irregularities in tooth shape or color may become more noticeable and may need correction through small composite additions or, in cases requiring more extensive correction, dental veneers.
No, the orthodontic appliance itself does not cause cavities, but it requires greater attention to oral hygiene at home. The appliance creates areas where plaque can accumulate, and if not removed, it can turn into tartar. However, the patient is regularly monitored by the specialist, who will provide instructions for proper cleaning
The main factors to evaluate are crowded, rotated, tilted teeth, spaces between teeth, and dental wear. However, improper occlusion between the dental arches (which may cause joint and muscle problems leading to headaches and neck pain) is not always recognizable by the patient.
Absolutely. Even in adults, teeth can be moved to achieve alignment that improves both function and smile aesthetics. What cannot be done in adults, unlike in children, is modify bone growth without surgical intervention.
The duration of orthodontic treatment depends on the severity of the malocclusion being corrected. It can vary greatly, ranging from a few months to 2–3 years. Follow-up appointments are scheduled with the orthodontist and vary according to individual circumstances.
At the end of orthodontic treatment, a maintenance phase is necessary to keep the results achieved. This can be done using a removable nighttime appliance or a fixed lingual retainer (a passive retainer applied to the lingual surface of the front teeth). The duration of this phase depends on the severity of the treated malocclusion, but the only way to ensure that alignment is not lost is to continue retention over time. In the case of removable retainers, the frequency of use can gradually decrease from every night to 3–4 nights per month or even less over time.
Yes, it is absolutely possible to correct an open bite with invisible lingual bracketless fixed orthodontics, although the effectiveness depends on the cause of the problem. This orthodontic technique can also correct diastema and other types of dental crowding. Invisible bracketless orthodontics is effective even in severe cases, unlike some invisible appliances that may not work in specific situations.
Invisible orthodontic treatment requires several technical components to achieve a successful result. Here is what you need to know to better understand this technique and, specifically, active retainers.
Other treatments considered “invisible” include lingual brackets and clear aligners. Among these, only lingual brackets can truly be considered invisible because they are attached to the lingual surface of the teeth and are therefore hidden from view. Clear aligners, on the other hand, create a visible film-like effect on the teeth, and the composite attachments bonded to the teeth — often necessary to optimize certain movements — are visible as well.
Choosing the right professional for bracketless lingual orthodontics (fixed but without traditional metal brackets) is a delicate step. This technique, often referred to as active lingual orthodontics, is extremely refined and requires a very different level of manual skill compared to traditional orthodontics.
Yes, it is absolutely possible to correct an open bite with invisible lingual bracketless fixed orthodontics, although the effectiveness depends on the cause of the problem. This orthodontic technique can also correct diastema and other types of dental crowding. Invisible bracketless orthodontics is effective even in severe cases, unlike some invisible appliances that may not work in specific situations.
Since this appliance is very thin and closely adapted to the teeth, the possibility of detachment is very low. If this does happen, there are two possible scenarios. The most common is a detachment without discomfort and without urgency to reattach it. Less commonly, detachment may cause discomfort, in which case the patient should bring forward their follow-up appointment or follow the instructions provided by the specialist if it is not possible to anticipate the visit.
Any patient with permanent dentition can undergo orthodontic treatment at any age. Teeth can always be moved provided there are no periodontal problems. Patients in the acute phase of periodontal disease must first undergo basic periodontal therapy as well as maintenance therapy during orthodontic treatment. All patients should undergo professional dental cleaning (tartar removal) before the appliance is applied and every 3–4 months during treatment, depending on the level of oral hygiene the patient is able to maintain at home.
Treatment time depends on the severity of the malocclusion and does not differ from traditional bracket-based therapies. The longest treatments usually last around two years and involve correcting severe misalignments, sometimes requiring tooth extractions or the recovery of impacted teeth within the bone.
Absolutely not. The wire bonding procedure is very similar to traditional bracket bonding procedures and is therefore carried out with full respect for the health of the teeth and gums. During the first days after activation, patients may feel pressure on the teeth, which is typical of any orthodontic treatment. This sensation is generally well tolerated and temporary.
Bibliographic references about bracketless fixed orthodontics.
1-Am J Orthod Dentofacial Orthop. 2014 Oct;146(4):411. Forces and moments generated by removable thermoplastic aligners: incisor torque, premolar derotation, and molar distalization. Simon M, Keilig L, Schwarze J, Jung BA, Bourauel C.
2- Angle Orthod. 2014 Nov 20. Efficacy of clear aligners in controlling orthodontic tooth movement: A systematic review. Rossini G, Parrini S, Castroflorio T, Deregibus A, Debernardi CL.
3- Orthodontics (Chic.). 2011 Winter;12(4):386-95. A segmented appliance for space closure followed by Invisalign and fixed appliances. Uribe F1, Cutrera A, Nanda R.
4- Am J Orthod Dentofacial Orthop. 2009 Jan;135(1):27-35. doi: 10.1016/j.ajodo.2007.05.018. How well does Invisalign work? A prospective clinical study evaluating the efficacy of tooth movement with Invisalign. Kravitz ND, Kusnoto B, BeGole E, Obrez A, Agran B.
5- Angle Orthod. 2007 Sep;77(5):864-9. Invisalign and traditional orthodontic treatment postretention outcomes compared using the American Board of Orthodontics objective grading system. Kuncio D, Maganzini A, Shelton C, Freeman K.
6- Prog Orthod. 2006;7(1):32-43. Extraction treatment using Invisalign Technique. Giancotti A, Greco M, Mampieri G.
7- J Am Dent Assoc. 2002 Mar;133(3):369-71. Orthodontics and the general practitioner. Christensen GJ.
8- J Orofac Orthop. 2005 Mar;66(2):162-73. Motivation, acceptance and problems of invisalign patients. [Article in English, German]Nedwed V1, Miethke RR.
9- Am J Orthod Dentofacial Orthop. 2005 Sep;128(3):292-8; discussion 298. Outcome assessment of Invisalign and traditional orthodontic treatment compared with the American Board of Orthodontics objective grading system. Djeu G, Shelton C, Maganzini A.
Do you want a truly invisible orthodontic appliance?
Contact us today to discover whether bracketless treatment is right for you. Request a personalized consultation and schedule your visit with our team. We support international patients with clear information and assistance before and during their stay in Naples. Leave your contact details and we’ll get back to you promptly.
- Phone: +39 081 245 1805
- Email: info@studiodentisticocozzolino.it
- Address: Via Raffaele De Cesare 31, 80132 – Naples, Italy

{kind=link}